
CNN vs Ivermectin
CNN says study shows Ivermectin does not work -- but it shows that it DOES

Came across this tweet from a bluecheck CNN anchor:
I was so sad to hear that Ivermectin is not effective, so I decided to give the study a closer look.
The study had a 241 person study group who received 0.4 mg/kg Ivermectin for 5 days, which is the FLCCC recommended dose. (my wife got 0.3 mg/kg). It also had a 249 person control group who received the standard of care. (and no ivermectin)
The patients were at-risk persons with comorbidities, most likely to get sick or die.
Design, Setting, and Participants The Ivermectin Treatment Efficacy in COVID-19 High-Risk Patients (I-TECH) study was an open-label randomized clinical trial conducted at 20 public hospitals and a COVID-19 quarantine center in Malaysia between May 31 and October 25, 2021. Within the first week of patients’ symptom onset, the study enrolled patients 50 years and older with laboratory-confirmed COVID-19, comorbidities, and mild to moderate disease.
Interventions Patients were randomized in a 1:1 ratio to receive either oral ivermectin, 0.4 mg/kg body weight daily for 5 days, plus standard of care (n = 241) or standard of care alone (n = 249). The standard of care consisted of symptomatic therapy and monitoring for signs of early deterioration based on clinical findings, laboratory test results, and chest imaging.
To my utter shock, the study actually showed that Ivermectin DID work:
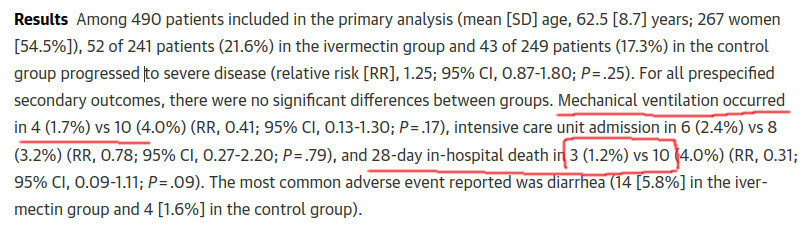
So, the study showed that , for Ivermectin vs control group:
4 vs 10 were placed on mechanical ventilation
3 vs 10 died (so 3 Ivermectin patients died, vs 10 without Ivermectin).
For those versed in statistics, the “statistical significance” of these differences (P) was 0.19 and 0.09. It does not get under the standard of P <= 0.05, so the difference can be called “not statistically significant”. But it IS significant to us, and the P values are high because the study was underpowered.
Clearly Ivermectin showed positive effect, 3 vs 10 deaths is a huge benefit. The study likely saved about 7 lives by giving Ivermectin to 241 persons.
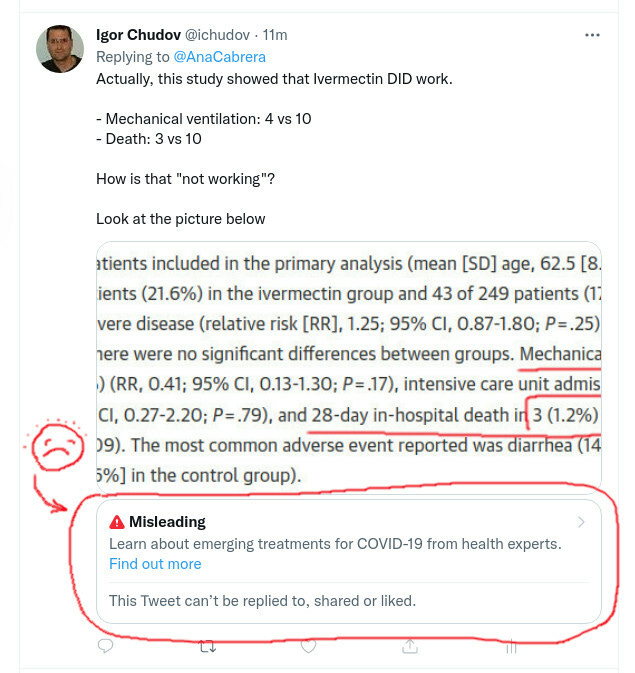
So I posted a tweet explaining the numbers from the article, and you know what happened? Take a look and sorry for my Hunter Biden-level art skills
Seriously, for fatality rate of 1-3%, clearly it is NOT enough to have such small 200-person study and control groups. Still, I am thankful to researchers who conducted this study and for saving approximately 7 people from dying by giving them Ivermectin.
Our astute reader Dean commented and his thinking about the P value is the clearest explanation I have ever seen:
If I understand correctly, "P= .09" means there is a 91% chance that the effect was not by chance. And if there's a 91% probability that by taking a harmless drug for a few days I can reduce my chance of death by 70%, then how stupid would I be to refuse? The P=.05 cutoff is arbitrary and doesn't take into account risk vs. benefit, right?
So, why does the article say Ivermectin did not work, where it clearly reduced the worst outcomes (ventilators and deaths)?
It is possible that their “conclusion” was a way to slip truthful real life numbers from JAMA anti-ivermectin censors.
Tempest on Substack
After writing this article, I had to visit a customer, and came back to find myself in the eye of a storm. It turned out that two more people wrote articles about this specific study:
Jessica Rose wrote a GREAT article about the same study. She made some good points about FLCCC dosing that I did not even think about.
Alex Berenson wrote a bombastic post titled Ivermectin fails, where he said that the same article that I and Jessica discussed, proves conclusively that Ivermectin is a failure. His post included only one paragraph of the study discussing “severe disease”.
I will not criticise him, but would note that the study was conducted IN HOSPITALS:
Design, Setting, and Participants The Ivermectin Treatment Efficacy in COVID-19 High-Risk Patients (I-TECH) study was an open-label randomized clinical trial conducted at 20 public hospitals and a COVID-19 quarantine center in Malaysia between May 31 and October 25, 2021. Within the first week of patients’ symptom onset, the study enrolled patients 50 years and older with laboratory-confirmed COVID-19, comorbidities, and mild to moderate disease.
Is it a wonder that people already in a hospital would soon require oxygen? How is that really a “primary outcome”? The “primary outcome” is death or other permanent adverse health outcome, not what happens a day after the person is hospitalized and given Ivermectin for the first time, and somehow the patient’s condition will improve in a day after hospitalization?
The feedback on Alex article’s comments is the most amazing.
If I understand correctly, "P= .09" means there is a 91% chance that the effect was not by chance. And if there's a 91% probability that by taking a harmless drug for a few days I can reduce my chance of death by 70%, then how stupid would I be to refuse? The P=.05 cutoff is arbitrary and doesn't take into account risk vs. benefit, right?
Another great example of undermining a real finding "the effect size" with an underpowered study "statistical significance." Do people ever do power analyses any more before they start a study, it was always required for any Ph.D. candidate.