
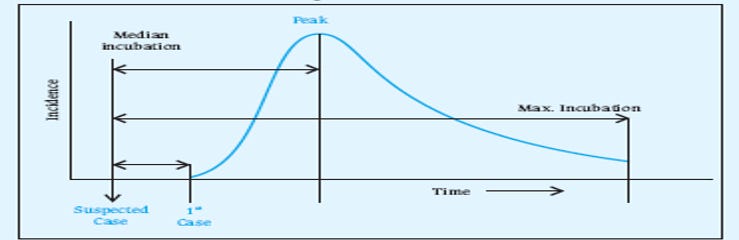
Mortality during explosive epidemic
Death rate doubles if the sick get no care

I hate being like CNN or MSNBC and to even utter the dreaded sentence “overwhelmed hospitals”. I feel like this is March of 2000 all over again, with the stupid talk that never materialized, and now I am suckered into the same discourse.
I wrote several separate articles about hospital utilization, how Covid is not to blame for current hospital capacity problems, how it is the vaxxed who are taking up hospital beds with colds from hell and heart problems, etc. So I am not out there waving the “hospitals are getting full” flag and begging people to take useless mRNA boosters.
But, at the same time, I try to be a realist and model reality. So let’s model Omicron for a minute.
Assume, for ease of calculation, that it reproduces in our society, without tyrannical lockdowns, at the rate of 10 times increase per week. The actual rate is probably close to that and may be 8 times per week or some such. We do not know the exact number and it is not important. What is important is that Omicron is very contagious and almost nullifies vaccine protections by evading Spike-antibodies. It also infects covid recovered, at about three times the usual reinfection rate (so perhaps 3-5%), according to one newspaper article.
If so, we can do a little modeling. It is easy for the beginning stage of the pandemic, which resembles an exponential curve. Note that the “epidemic curve” always eventually starts bending down and resembles a “bell”, but the beginning looks exponential.
This is how Omicron wave looks like:
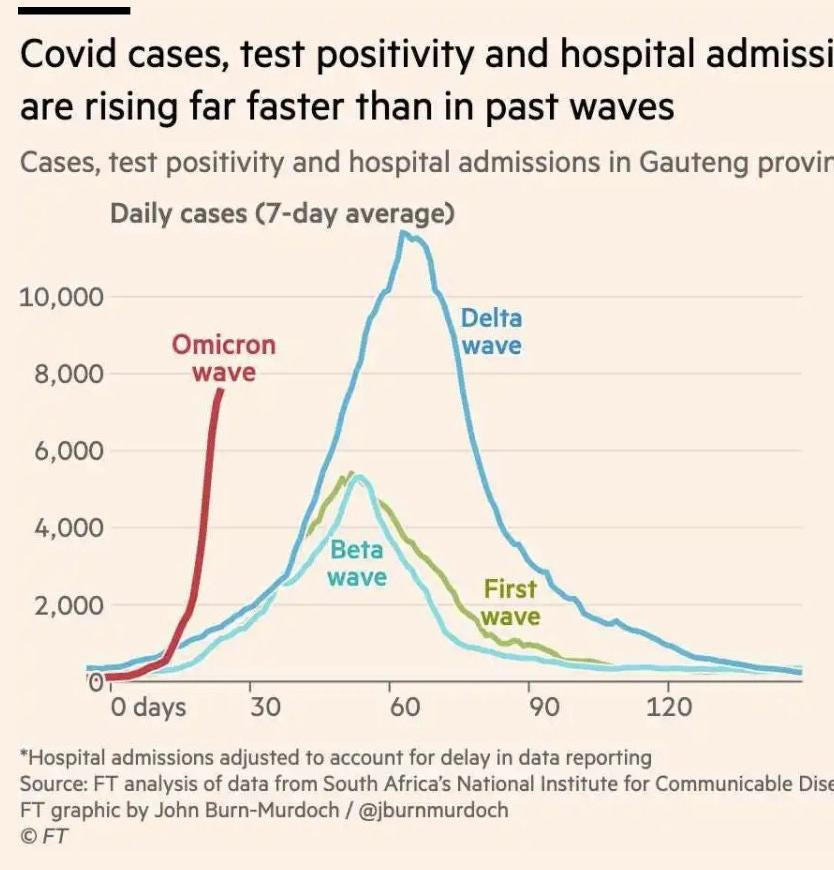
So you can see that it rises FAR more steeply than the previous waves.
Making a crazy assumption, for a moment, that we do not change our behavior and do not get locked down, this kind of growth rate puts us into uncharted territory.
For example, let’s say that today, December 8, 2021, we have 1,000 cases of Omicron in the USA. A week later, we will have 10,000, another week later 100,000 and in three weeks (by New Year) it will be a million total cases. Growing by about 40 percent per day, this would be 400,000 new cases per day. A week later it is 4 million cases per day.
Again, this is just a little numbers exercise to get a feel of the scale of the problem. Without a doubt, some attempts will be made to “lock down”, which might slow down the pandemic, perhaps, to about 3 times per week growth.
In any case, it is clear that in 4 weeks, we will have a big pandemonium, with the number of sick exceeding anything that we experienced.
In my earlier article, I said that Omicron may be twice as deadly as Delta. But that is assuming “all things being equal”, specifically that Omicron patients get hospital care as the Delta patients do right now. You can put forth a good case that Covid patients are not treated well, are not given proper early treatments or even proper late treatments. And you would be totally right.
But even with what we have, the number of Delta deaths would be probably double if Delta patients could not receive any hospital care. With the Omicron patients, if hospitals get actually overwhelmed (and extra beds will not help if there is no personnel), the fatality rate can easy double over what it would be with adequate medical care.
Earlier I described possible US fatality rate from Omicron as 2.5-3.2%. But that’s assuming people get cared for medically.
So a million of sick patients who fell ill on a particular day, who are not getting medical care, could end up having double the fatality rate — such as 5% fatality rate. This means, shockingly, that out of the 1 million sickened on this day, 50,000 people would die on average two-three weeks later.
Even a 2% fatality rate would translate into 20,000 deaths per day. To remind you, during the worst of the last winter pandemic, we would lose 4,400 persons per day maximum. Here we are talking about numbers an order of magnitude higher.
Important: almost no projections such as the above ever come true. They either come way below, or very rarely way above. There are very powerful reasons why we may not see crazy numbers like 20-50,000 casualties per day: the most important reason is that people get scared and hide out at home, or are mandated to. This slows the infection rate down.
However, we need to be supplied with food, electricity, trucking, fuel, etc and at least a half of all workers (the “essential” ones) have to work unless we want dire economic collapse. And essential workers have families. In addition, everyone is tired of the pandemic, lockdowns, etc. Fatalistic attitudes abound, including in your humble servant. I shopped maskless at my local Walmart today. People still want to visit friends, work, date, shop etc.
Thus, we cannot lock everyone down and so the epidemic growth rate will at best be a half of uncontrolled rate. Lockdowns cannot stop something as contagious. We will talk about lockdowns and “policy responses” later. And even if the rate of growth is a half (5 per week), the results will be similar. The point of this article is to underscore that something so extremely contagious can lead to fairly calamitous short term consequences as described.
The most dangerous aspect of Omicron is that it appears to be extremely airborne, sort of like chickenpox. If so, persons living in multifamily housing will likely NOT be able to hide out at all.
This means that, whatever the growth rate, if vaccinated and Covid-naive people are unprotected and covid recovered are only somewhat protected, we are in for a very wild ride of unknown magnitude.
Again, this is not a reason to despair, we were through worse pandemics such as smallpox in South America, or the plague in the Middle Ages. But we might see crazy death numbers like 20-50,000 deaths per day and feel like these people:
Igor, you need a break! This Omicron is a non-event. They just whipped it up to push the items on their list (lockdowns and compulsory vaxx in EU, boosters everywhere, 4th jabs). Omicron was circulating in Africa for months before they declared it on Nov. 23rd. And did Africa die? No. Why then? Because on that day SA changed in Covid-19 case counting rules so that an artificial spike in cases would ensure, everyone knew that. And do not trust all data they publish. They lie to us every day many times over, the bigger the lie, the more believable: "They couldn't have made it up!" Yes they can. They have no remorse or conscience. Don't fall for it. Any numbers they publish - it's their numbers. Remember Pfizer? Their trial data? Just like that. Now it will take FDA 75 years to publish that? And you still believe them? STOP!
Please quit parroting the omicron lie.
What is happening is that people's immune systems are being damaged by the experimental injections. Their bodies are thusly more susceptible to all manner of disease. This will worsen and Pharma will roll through the Greek alphabet to explain it away and continue with the fear mongering.
The average age of a death by or with "Covid-19" is higher than life expectancy in all Western countries. No other figure even need be known to understand the "pandemic" (business model) is a fraud and a giant Ponzi scheme.
The fact that there is no such thing as a "Covid death" is another minor problem here as SARSCoV2 itself is a computer generated fiction.
In the US the "Covid death" number is cooked/manipulated due to how the CDC does their accounting as well as many other factors- an audit of the CDC mortality numbers themselves is required.
1) The first thing that must be addressed is "who were these people?" The average age of a "Covid death" is 80 in the US and 82 globally w/4 comorbidities on average. The vast majority of these people were from nursing homes, assisted living, hospice etc. Where did the vast majority of initial "Covid deaths" occur? Here in the US (and everywhere in the West- Milan, Madrid, London, Brussels, Montreal, Toronto, etc.) most, if not all, who died from "Covid" already had one foot in the grave and their death was put on fast forward through medical protocols not an anomalous viral event.
What we had here in the US was a radical and mandatory shift in policies relating to hospitals, care homes and the overall social order. These new "policies" were mandated through various new and aberrant state "guidelines" which resulted in a concentrated death rate for a six week period in March/April. Take that out of the equation and there is no death rate to talk about. Put (or keep) these policies in place and we will have this happen every year.
There was also gross negligence (beyond the usual) in numerous nursing homes that led to abandonment and medication alterations that turned these slow motion abattoirs into death houses. One of the remarkable things of note is that here in the US the "pandemic" was not widespread (which is supposed to be one of the defining features of a pandemic) but was in fact limited to very specific locations;
2) The faulty diagnosis of what is a "Covid death" did they die "with" or "from" Covid which is problematic for several reasons. In many cases an actual test was never done only a "presumed to be Covid" assessment was put forth. Add to this that when the tests were done PCR tests done with faulty specs (gene sequencing, cycle thresholds, annealing problems, faulty primers and so forth) were used. PCR can't diagnose anything in the first place and compounded with these problems they are useless and misleading;
3) No autopsies. Why were no autopsies done in the US? Why did they pass new mandates that halted all autopsies for "Covid deaths?" This went against decades long protocol. They also changed decades old protocol on how death certificates should be filed;
4) Another way they inflated death counts was through hospital admissions and faulty PCR testing. So for example if one came in with a coronary condition you would be given a "Covid test" no matter what- all admissions required this- and then if you died while in the hospital you could have been listed as a "Covid death." This happened frequently throughout the year;
5) Home deaths is yet another way that figures were cooked. This was admitted point blank by Stephanie Buehle (NY Dept. of Health spokesperson) among others who stated that home deaths with no testing at all would be presumed "Covid deaths." This "guideline" was mandated through the NY Health Dept;
6) "Covid death counts were forged- CDC instructed officials to certify any death as "caused by" COVID if the decedent tested positive prior to passing or was suspected of having "C19", even if it wasn't the actual cause of death. Thus we have major misattribution. E.g., we have over 14,000 injury deaths listed in the "C19 death" total.
We also unexplained declines in other common death categories because so many have been attributed to "C19." The unprecedented broad definition of "C19" death has created huge fraud in "Covid death" counts;
7) Another way they inflated death counts was through hospital admissions and faulty PCR testing. This caused a huge spike in iatrogenic deaths caused by misattribution of "Covid" to incoming patients and the ensuing improper treatments applied e.g. ventilators, remdesivir and associated fentanyl dosages which killed thousands.
So for example if one came in with a coronary condition you would be given a "Covid test" no matter what- all admissions required this- and then if you died while in the hospital you could have been listed as a "Covid death." This happened frequently through the year.
The practice of PCR-testing hospital admissions who are asymptomatic for Covid using high Ct values undoubtedly caused deaths and unnecessary suffering.
This matters for several reasons. A pneumonia patient e.g. has a very good chance of surviving with correct support. However, if the patient tests ‘+’ for the non-existent pathogen an entirely different medical protocol goes into action and with this and there is little chance of survival.
The 'diagnosis' of "Covid" effectively permits dangerous protocols to be enacted that then increase the chance of mortality.
With regard to adoption of a new RT-PCR protocol for hospital admissions this also falsely manufactured death statistics for "Covid." Add to this how it was incentivized-$$$$$ while hospitals are under extreme financial duress. The US hospital system had it's worst financial quarter on record in the middle of a "pandemic." Administrators were under pressure to alleviate that financial pain and exploit all openings in the CARES Act.
None of this is accidental.
8) Lockdown impacts- too numerous to cite here.
In short whatever "excess deaths" which may have occurred anywhere can be attributed to people who didn't have to die but were KILLED due to the unnecessary use of ventilators, harsh toxic drugs, people dying prematurely do to lack of medical treatment, ill effects from the lockdowns and so on.