
Pfizer's RSV Vaccine Math: Kill 4,000 Newborns to Save 300 from RSV
Welcome to the New Woke $$$$ Math

Respiratory Syncytial Virus, or RSV, is a widely circulating respiratory virus that causes colds. This virus came from a lab around 1955 when scientists were researching monkeys at the Walter Reed Army Institute, but since then, it has been endemic to humans. The first encounter with RSV is the worst, and some babies get pretty sick.
The history of RSV vaccines has been marked by sixty years of failure due to the first RSV vaccines making the infection worse instead of better, with two vaccinated infants dying in a small trial.
Encouraged by the COVID-given ability of pharmaceutical companies to sell untested vaccines targeting pregnant women, both GSK and Pfizer set out to create a new, prefusion-stabilized antigen RSV vaccine (not based on mRNA technology) for expectant mothers. EDIT: in her post published shortly after mine, Meryl Nass explains that the stabilized antigen was developed by the NIAID and given to both Pfizer and GSK.
GSK and Pfizer’s RSV vaccines are nearly identical in composition.
Both vaccines, when given to pregnant mothers, cause an increase in premature births and infant deaths.
Both vaccines - which are almost the same composition - cause an increase in preterm births equal to about 2% of all births:
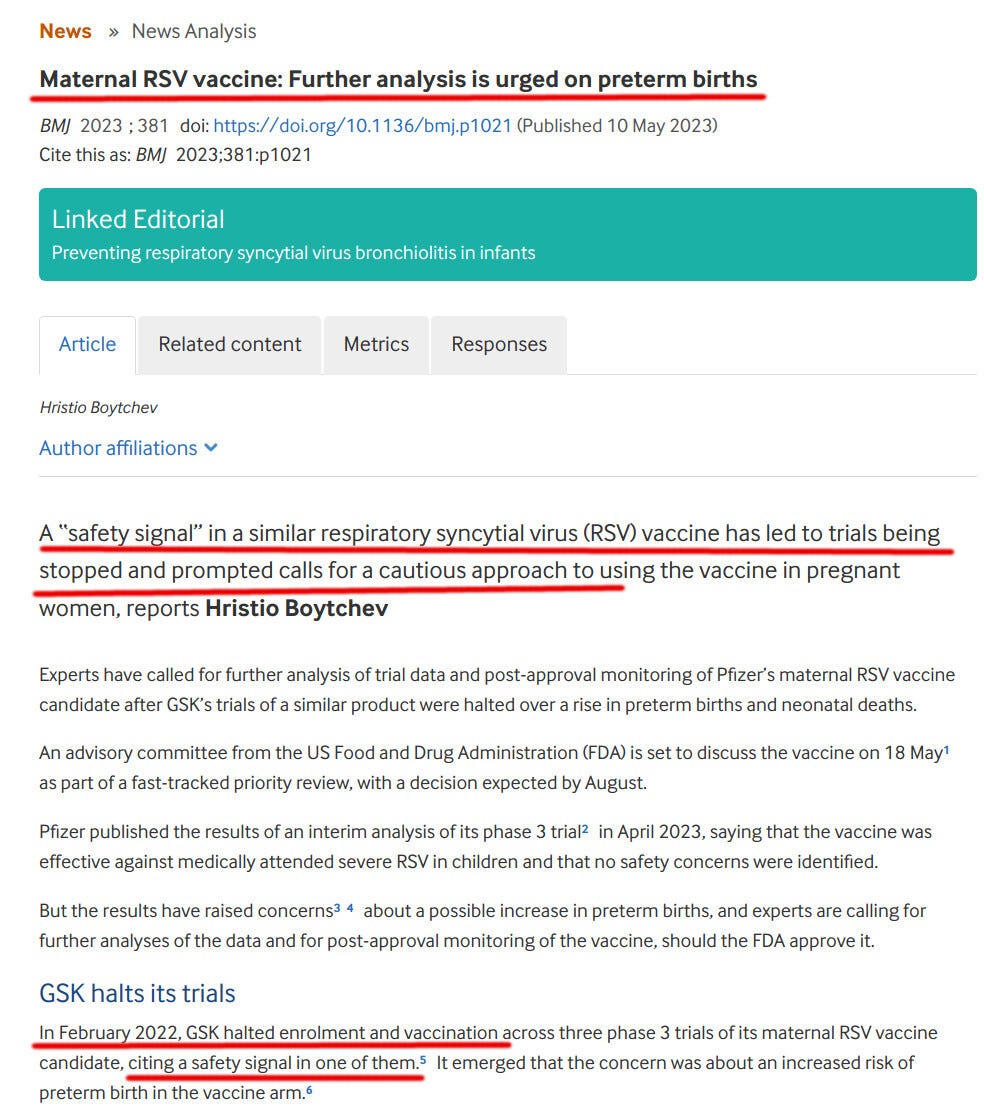
In a document submitted to the FDA, GSK’s data showed 238 preterm births out of 3496 (6.8%) in the vaccine arm and 86 out of 1739 (4.9%) in the placebo arm—around one extra preterm birth for every 54 vaccinated mothers. There were 13 neonatal deaths in the vaccine arm and three in the placebo arm.
Differences in preterm births are evident in Pfizer’s RSV trial. In adverse event tables for its phase 2 study, published in October 2022, Pfizer reported 3 out of 116 (2.6%) premature births in the placebo group and 6 out of 114 (5.3%) in the group that received the vaccine that was chosen as Pfizer’s final product.
As a company long-established in the field of vaccines, GSK decided to pull its product due to safety concerns. Despite having essentially the same product, Pfizer insisted on getting its RSV vaccine approved.
Pfizer refused to answer safety questions or explain why its vaccine is so different as to have a better safety profile compared to GSK’s:
Pfizer did not respond when asked about a possible increase in preterm births associated with the vaccine in its two trials, but told The BMJ that “no imbalance of neonatal deaths was observed” in its phase 3 trial.
Both the FDA and the CDC decided to ignore the safety signal of increased preterm births, and the CDC now recommends it to all pregnant women.
The CDC’s tweet leads here:

What would happen if the RSV vaccine was given to all pregnant women in the United States? Would it prevent deaths or cause more deaths?
Let’s gather some numbers, all coming from the CDC:
In 2021, 3,664,292 births were registered in the United States
An estimated 58,000 to 80,000 children under five years of age, mostly infants, are hospitalized annually nationwide due to RSV infections.
Annually, 100 to 300 children younger than five die due to RSV.
All my calculations below will give the maximum benefit of the doubt to the numbers supplied by the CDC. The imbalance they show will shock you; there is no need to question them to make my point.
An increase in preterm births of 2% would lead to 3,664,292*0.02 = 73,285 additional preterm births.

As most readers know, preterm births are dangerous and lead to greater infant mortality. Indeed, this is what the study by GSK saw (Pfizer’s study included fewer subjects and could not reliably count infant deaths due to its smaller size):
In a document submitted to the FDA, GSK’s data showed 238 preterm births out of 3496 (6.8%) in the vaccine arm and 86 out of 1739 (4.9%) in the placebo arm—around one extra preterm birth for every 54 vaccinated mothers. There were 13 neonatal deaths in the vaccine arm and three in the placebo arm.
Ilse Dieussaert, vice president of vaccine development at GSK, said that the increase in neonatal deaths was because of deaths in premature babies and that there was no imbalance of deaths in full term babies.
The GSK’s vaccine arm (3496) was twice as big as the placebo arm (1739), so the vaccinated/unvaccinated death ratio is 13:6, not 13:3. Still, the deaths have a worse than 2:1 imbalance (13:6), disfavoring the vaccinated group!
How many RSV hospitalizations of infants could be prevented by Pfizer’s RSV vaccine? At most, it would be about 57% of total hospitalizations of kids under 5, or between 58,000*0.57 to 80,000*0.57, or between 33,060 and 45,600 total hospitalizations.
In other words, Pfizer’s RSV vaccine would cause MORE premature births (73 thousand) than it would prevent RSV hospitalizations!
Consider, also, that anything causing premature birth is likely to damage the developing fetus.
Almost no child dies from RSV (see the above quote of 100-300 children under five dying of RSV, coming from the CDC). So, we must weigh the deaths caused by premature births versus, at most, 300 lives saved by the Pfizer vaccine!
How many infant deaths could be caused by the Pfizer vaccine? Consider that the infants of vaccinated mothers in the GSK trial, which was sufficiently powered to see some infant deaths, died at a greater rate of 13:6 (116% increase) compared to the placebo infants.
So, Pfizer’s RSV vaccine could double the infant death rate. We have a relatively small amount of data (which is why this vaccine should not have been approved or recommended), but let’s assume that infant mortality would be increased by only 20%, not 116%. This makes the calculation more conservative and defensible.
The US sees about 20,000 infant deaths annually:
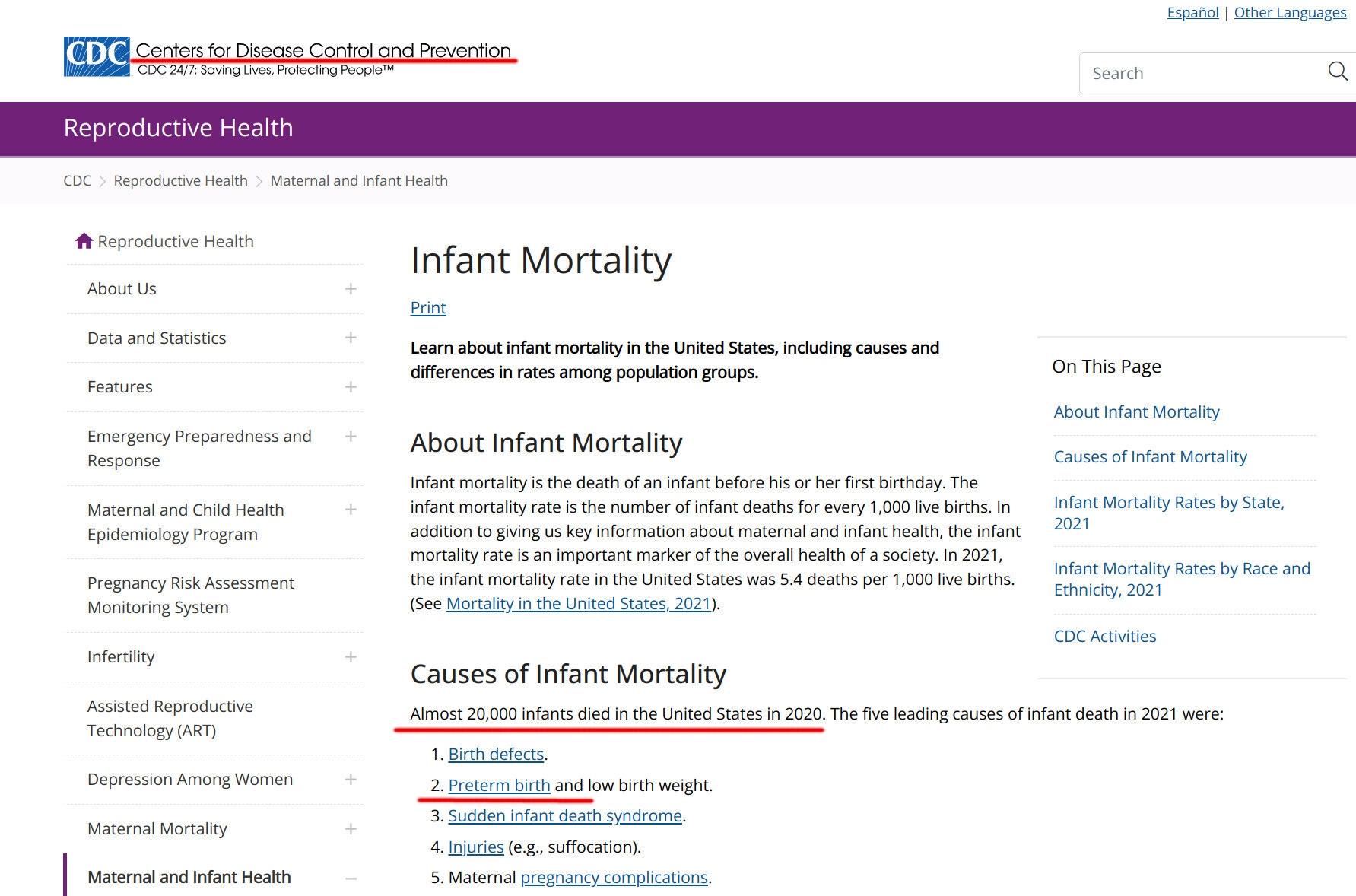
The above assumptions mean that in addition to the 20,000 infants who die yearly for various reasons, an additional 20%, or 4,000, would die due to Pfizer’s RSV vaccine.
So, 4,000 infants would die from Pfizer’s vaccines to save fewer than 300 infants from RSV.
Please help me make sense of this!
How would you approve a barely tested vaccine whose almost identical withdrawn counterpart caused a 13:6 ratio of infant deaths in a clinical trial?
How can saving at most 300 lives justify endangering 4,000 (or more) lives?
My calculation is, necessarily, imprecise. But there is such a massive imbalance between the vaccine downside (deaths due to premature births) and the tiny possible upside that I cannot imagine any rational reason to approve this vaccine.
I mean, it could not be the money from Pfizer, right?
What would possess any mother of a newborn to submit her baby to be a test subject for untested vaccines?? Seriously! I can’t wrap my head around how any mother would allow her baby to be used, and possibly poisoned/killed like this! There’s no financial remuneration large enough to even remotely make this ethical, moral, or simply the actions of a loving mother.
Here is how I think the fed public health officials cut this Gordian knot--the preemies due to vaccination. They reduced the window of time during which a mom should be vaxxed to 32-36 weeks' gestation. They called all babies born after 36 weeks full term. Thus there will be many fewer preterm birth.
Beware, however, because Moderna has an RSV mRNA candidate waiting in the wings.
Also, CDC's claims about how may babies die of RSV is a fantasy. CDC published a paper in 2021 showing that only 25 babies yearly die with RSV and 17 die from RSV--according to death certificates. I see that I had better post my RSV slides.