
UK Data shows the Vaxxed are Superspreaders
And "protection from death" keeps dropping

This post is a weekly update on “UK Vaccine Hell”. My First post that started this series was viewed over 16,000 times and seems to have found its way across social networks. Please read it BEFORE you read the rest of this document, to understand my methodology.
My first article shows that vaccines in the UK are not only not effective when it comes to preventing cases of Covid19, but in fact they have the opposite effect of ATTRACTING Covid19 and making vaccinated case rates much HIGHER, oddly, than the unvaccinated. Can someone help me with finding an antonym (word with opposite meaning) fo “effective”. It is not “ineffective”, it is a word that would mean “worse than ineffective”. Counterproductive, maybe?
My next update from last week showed deepening of UK vaccines’ tendency to make the vaccinees attract Covid19, such numbers as 40-49 vaxxed group being 2.24 TIMES more likely to attract Covid, and all groups besides the youngest afflicted.
This Week’s Cases
“Worse than ineffective” now rules this current report. Well, this week ‘s new PHE vaccine effectiveness report, predictably looks much worse than even last week’s. I am running out of dramatic adjectives and we are quickly moving from tragedy down into the comedy realm. All Age groups above 30 show grossly negative effectiveness against disease. The vaxxed in the 40-49 group are 2.32 TIMES more likely to catch Covid, than the unvaccinated. Wow
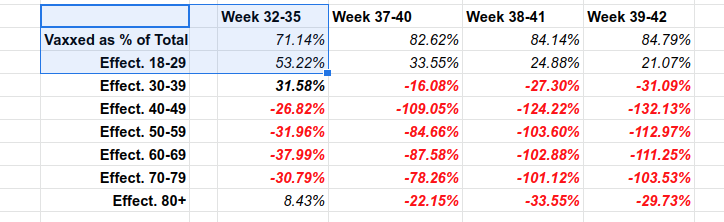
Now, being unvaccinated is protective from catching covid and being vaccinated is inviting Covid. The vaccinated are the superspreaders of the disease and a threat to the UK society (which is mostly vaccinated, so you cannot isolate them).
This Week’s Deaths
I must say this out loud: THERE IS STILL PROTECTION FROM DEATH FOR THE VACCINATED. This is one more reason why I called them superspeaders: they get infected and spread the disease, at a lower (although constantly rising) personal cost in terms of death.
However, every week, the protection from death continued its’ decline.

The decline is somewhat slower than the previous week, but still the vaccines are less and less protective from dying. The 18-29 age group has so few deaths, that death numbers are highly variable week to week and do not tell us much. I would not overdramatize 16% decline among youngsters, as it is likely just a statistical fluke. For all other age groups other than 40-49, protection showed further slide downwards.
Disclaimers and Quality of Data
I would like to express my enormous gratitude to PHE for publishing such explosive materials and for being truthful with its data. I am sure that PHE’s leadership is under incredible pressure to withhold numbers.
The corporate UK media is already complaining how PHE’s data is being “exploited by antivaxxers”. Well, of course it is, since it shows that vaccination is a total failure! And yet, PHE continues to supply us with high quality, truthful data. Thank you PHE!
Let me explain why that data is so high quality: by counting all deaths within 28 days of Covid diagnosis, PHE overstates covid deaths for all categories, but at the same time is completely consistent and compares “apples to apples”. It also does not depend on “cause of death reporting” by hospitals. All of this data is fudged in the US, leaving us with fake CDC statistics.
The counts of vaccinated vs unvaccinated, using NIMS data, are also highly reliable as they include specific names and their vaccination status. The percentages of the vaccinated are not changing much any more, what is driving all this drama is rapidly changing case rates.
PHE states directly to NOT use this data to calculate vaccine effectiveness. It says:
Comparing case rates among vaccinated and unvaccinated populations should not be used to estimate vaccine effectiveness against COVID-19 infection. Vaccine effectiveness has been formally estimated from a number of different sources and is described on pages 4 to 7 in this report. The case rates in the vaccinated and unvaccinated populations are unadjusted crude rates that do not take into account underlying statistical biases in the data.
While they have some point in that various confounders can be endlessly discussed (who is more likely to wear masks? who is more sickly? who is unemployed? who works from home?), the data itself is so stark, that none of these adjustments is likely to make a huge difference in conclusions.
What does the future hold?
Predicting the future is extremely hard. Predicting future of Covid is even harder. So instead of predicting what will happen, I will pose some questions and some points:
In the absence of boosters, everyone in the UK will get Covid eventually. If boosters are used, it is not certain that Brits will survive repeated and more and more frequent application of boosters, or whether boosters will stop working at all. This is not known to anybody. You would need boosters, shots for variants, boosters for variants, and more and more frequent shots destroying what is left of Brits immune systems, and giving rise to new variants.
It is possible, but not certain, that the vaccinated, due to miswiring of the immune system, may not be able to acquire natural immunity the same way the “normal”, unvaccinated people do, and will catch Covid repeatedly. Instead of forming a wide array of antibodies and memory cells, the vaxxed seem to just make more of the worthless spike antibodies. Whether this will come to fruition or not, is NOT KNOWN. This was discussed at length by Alex Berenson and Eugyppius.
Introduction of boosters will muddle the picture. Who is now called the “unvaccinated”? Will there be a separate category for the boostered? If not, will the boostered artificially improve the statistics for the vaccinated for a couple of months while extra antibodies are still in the system?
Will the PHE stop publishing numbers that are so embarrassing to the UK vaccinators?
mRNA shots and boosters are NOT harmless, consequence-free injections like vitamin shots. They short circuit our body’s most innate genetic machinery (mRNA expression), most innate immune responses (spiking our blood with free floating spike proteins unconfined to the shoulder muscle), they contain nanoparticles designed to fool our immune system, etc. Thus, their application, and repeated application, may seriously alter the Brits most basic bodily physiology. There are already disturbing reports of "colds from Hell" sending Brits to hospitals and may other indications that something is seriously wrong.
It is possible that the vaccinated, due to the above reasons, will be absolutely left with no choice but to use booster injections until they die, vs dying right away, due to destruction of their innate immune system. It is great news for Pfizer and Moderna’s shareholders, until said shareholders physically die off.
The UK is NOT Unique and not “Bad”
Please note that even though we discuss "UK vaccination failure" and such, it is not because somehow, the UK is a uniquely bad country. Not at all. The UK is not unique at all and not bad in any way.
The only reason why we discuss is that UKHSA is extremely honest and extremely diligent in collecting relevant data, so we have honest data. The same disaster where heavily vaccinated countries experience a wave f Covid and deaths among the vaxxed, occurs in other places, possibly at differing stages of the same process. It is just not as honestly reported as the UK.
About me
I am not a scientist. I do not own a lab or a scientific institute. However, I own a brain and no one else owns my brain. I have two degrees (computer science and business) and I have every right to make up my own opinion and share it. You are free to agree or disagree with me.
Thank you, Igor. I wish everyone would read this. Sigh.
http://www.eecs.qmul.ac.uk/~norman/papers/inconsistencies_vaccine.pdf